
Claim Page 03 – Entering a Notice of Termination/Revocation – NOTR (8XB)
Claim Page 03 (MAP 1713) contains payer information, diagnosis code information, and physician information.
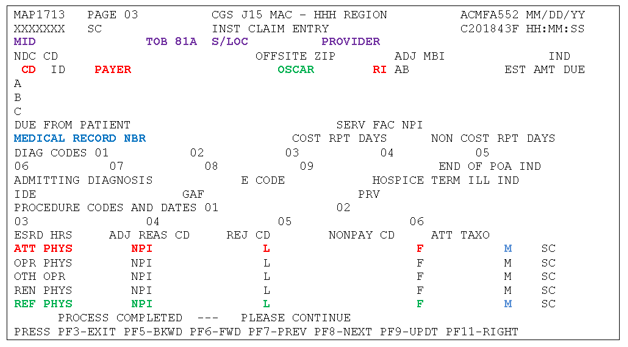
Key:
- RED = Required field
- BLUE = Optional field
- GREEN = Conditional field, dependent on the type of claim
- PURPLE = System generated field
- BLACK = Not required field
Field Descriptions for NOTR Page 03 – MAP 1713
Field Name/Requirement |
UB-04 Form Locators (FL) |
Description |
|---|---|---|
CD |
N/A |
Enter "Z" on line A. |
PAYER |
FL 50 |
FISS Will automatically plug "Medicare" into this field. |
RI |
FL 52 |
Release of information. |
MEDICAL RECORD NBR |
FL 3b |
Beneficiary's medical record number. |
ATT PHYS NPI |
FL 76 |
Enter the NPI of the patient's attending physician. If the patient does not have an attending physician, enter the NPI of the certifying physician. |
L |
FL 76 |
Enter the last name of the attending physician. If the patient does not have an attending physician, enter the last name of the certifying physician. |
F |
FL 76 |
Enter the first name of the attending physician. If the patient does not have an attending physician, enter the first name of the certifying physician. |
M |
N/A |
Enter the middle initial of the attending physician. |
REF PHYS NPI |
FL 78 and 79 |
Enter the NPI of the physician responsible for certifying the patient as terminally ill, if different than the attending physician. |
L |
FL 78 and 79 |
Enter the last name of physician responsible for certifying the patient as terminally ill, if different than the attending physician. |
F |
FL 78 and 79 |
Enter the first name of physician responsible for certifying the patient as terminally ill, if different than the attending physician. |
M |
N/A |
Enter the middle initial of physician responsible for certifying the patient as terminally ill, if different than the attending physician. |
Additional FISS Claim Pages
- Notice of Elections (NOEs)/Transfer NOE
- Hospice Claims
- Notice of Election Termination/Revocation (NOTR) – 8XB
Updated: 04.16.2021
