
Claim Page 01 – Entering a Notice of Election (NOE)/Transfer NOE
The following information provides guidance on how to enter these billing transactions in the Fiscal Intermediary Standard System (FISS) Claims/Attachments option (FISS Main Menu option 02) via Direct Data Entry (DDE). The corresponding UB-04 Form Locator (FL) is also identified. NOEs may be submitted via Electronic Data Interchange (EDI). Refer to CMS 837I NOE Companion Guide![]() for the required elements.
for the required elements.
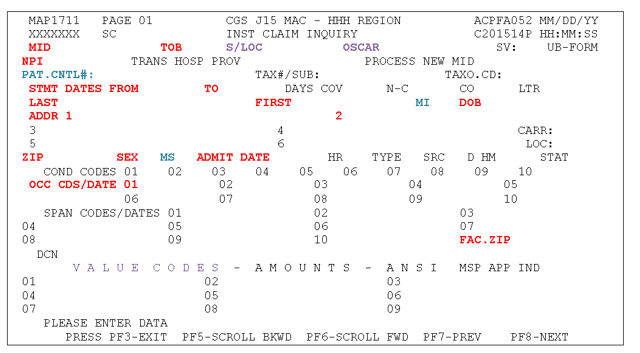
Claim Page 01 (Map 1711) contains general patient information, condition codes, occurrence codes, occurrence span codes and value codes.
Begin entering data on Claim Page 01 and continue until the necessary fields are completed. Use the key and table below to determine what fields are required and what information to enter.
Note: The codes listed on this page represent those most frequently submitted on hospice claims. A complete listing of all codes is accessible from the National Uniform Billing Committee (NUBC) Official UB-04 Data Specifications Manual![]() .
.
Key:
- RED = Required field
- BLUE = Optional field
- GREEN = Conditional field, dependent on the type of claim
- PURPLE = System generated field
- BLACK = Not required field
Field Descriptions for Claim Page 01 – Map 1711
| Field Name/Requirement | UB-04 Form Locator (FL) | Description |
|---|---|---|
| MID Required |
FL 60 | Enter the beneficiary's Medicare ID number |
| TOB Required |
FL 4 | Type of bill (system generated). FISS Page 01 defaults the type of bill (TOB) to 81A. You may need to change this depending on the TOB you are entering. 1st Digit 8 – Hospice 2nd Digit 1 – Hospice (nonhospital based) 2 – Hospice (hospital based) 3rd Digit A – Admission/Election Notice C – Change of Hospice Provider (i.e. hospice transfer) |
| NPI Required |
FL 56 | Enter your National Provider Identifier. |
| PAT.CNTL# Optional |
FL 3a | Up to 20 digits are available for you to enter your internal account number for tracking purposes. This number will display on your Remittance Advice or your Electronic Remittance Advice |
| STMT DATES FROM Required |
FL 6 | Enter the FROM date of this hospice election or the date of hospice transfer in MMDDYY format. A TO date is not required on NOEs. |
| LAST Required |
FL 8 | Enter the beneficiary's last name exactly as it appears on the Medicare card or the beneficiary's eligibility file, including any spaces, apostrophes, hyphens or suffixes. |
| FIRST Required |
FL 8 | Enter the beneficiary's first name exactly as it appears on the Medicare card or the beneficiary's eligibility file. |
| MI Optional |
FL 8 | Enter the beneficiary's middle initial. |
| DOB Required |
FL 10 | Enter the beneficiary's date of birth. |
| ADDR 1-6 Required |
FL 9 | Enter the beneficiary's full mailing address, including street name and number, post office box number or RFD, city and state. |
| ZIP Required |
FL 9 | Enter the beneficiary's 5- or 9- digit zip code. |
| SEX Required |
FL 11 | Enter the beneficiary's sex using the appropriate alpha character. M = Male F= Female |
| MS Optional |
N/A | Beneficiary's marital status |
| ADMIT DATE Required |
FL 12 | Enter the effective date of the hospice election or date of hospice transfer. |
| COND CODES Conditional |
FL 18-28 | Condition codes are not required on an original NOE. Condition code D0 is reported when a hospice is correcting an election date. NOTE: Occurrence code 56 must also be reported. Refer to the Claim Page 01 – Correcting a Notice of Election (NOE) for additional information. |
| OCC CDS/DATE Required |
FL 31-34 | Occurrence code 27 and the date of certification. This date must match the FROM date and ADMIT DATE, except for transfer NOEs. An occurrence code 27 is not required on a transfer NOE, unless the date of transfer is also the first day of the next benefit period. |
| FAC.ZIP Required |
FL 1 | Facility zip code of the provider or the subpart (9-digit). |
Additional FISS Claim Pages
- Notice of Elections (NOEs)/Transfer NOE
- Hospice Claims
- Notice of Election Termination/Revocation (NOTR) – 8XB
Updated: 04.14.21
