
IRF ADR Checklist
CGS recommends providers organize the medical documentation in the order indicated below. This will assist CGS in reviewing your documentation more efficiently and will expedite the review process. Please ensure the documentation is submitted within 45 days of the Additional Documentation Request (ADR). If the documentation has not been received, the claim will automatically deny on the 46th day for non-receipt of documentation.
Providers should submit all documentation that is pertinent to support the medical necessity of services for the billing period being reviewed. Ensure services billed are coded accurately for the service provided and the documentation supports those services. This may include documentation that is prior to the review period, such as an Individualized Treatment Plan (ITP). Please note that the most common reason for overturned appeals are due to providers submitting new documentation upon the appeal that was omitted with the initial submission of medical records.
*Please include the beneficiary name and date of service on all documentation and include an abbreviation key (if applicable). Documentation must be legible and complete (including signature(s) and date(s)). If you question the legibility of your signature, you may submit a signature log or an attestation statement.
The Checklist below is intended to be utilized by providers as a reference when responding to Additional Documentation Requests (ADR) to ensure each claim meets the policy requirements prior to the ADR submission. Please submit all documentation as required in the LCD or NCD if applicable and in accordance with the Medicare Benefit Policy Manual. It is the responsibility of the provider to submit complete and accurate documentation per the regulatory guidelines for each claim. Ensure the documentation submitted belongs solely to the intended beneficiary and documentation of another beneficiary is not present within any aspect of the medical record.
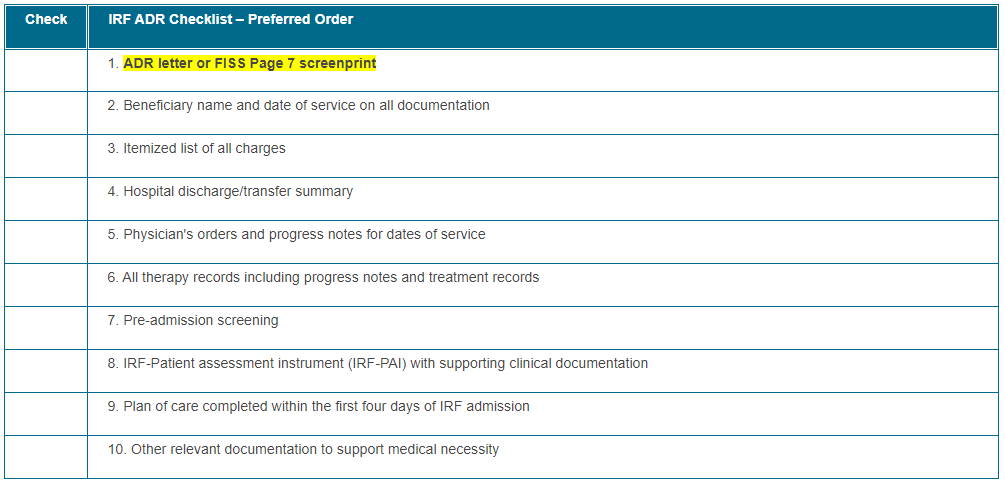
Click on the table below for a printable version.
The following resources may be used to ensure complete and accurate knowledge of the various Medicare benefits and billing requirements associated with this review:
Helpful Links:
- Medicare Benefit Policy Manual Ch 1- 110 – Inpatient Rehabilitation Facility (IRF) Services

- CMS Medicare Program Integrity Manual (Pub. 100-08), Chapter 3, Section 3.3.2.4
- CMS MLN Matters Article MM6698, Signature Guidelines for Medical Review Purposes
- Definition of "medically necessary": Social Security Act (SSA), Section 1862 (a)(1)(A)

- CMS Inpatient Rehabilitation Facility PPS
- CMS MLN Educational Tool: Medicare Payment Systems
- MLN905364 – Complying with Medicare Signature Requirements
- Electronic Code of Federal Regulations
- Medicare Claims Processing Manual Chapter 3 – Inpatient Hospital Billing
- Medicare Provider Compliance Tips – IRF
How to Prevent Common Denials:
Ensure the medical record is submitted within 45 days of the Additional Documentation Request (ADR) and the documentation includes all required policy components.
* The patient's (pt's) condition must be such that there is a reasonable expectation at the time of admission that the pt will be able to actively participate in and benefit from the intensive IRF program.
Ensure Documentation includes:
- Orders must be signed and dated legibly. If the physician/non-physician practitioner (NPP) (e.g. PA, APRN) signature is not legible or signed electronically, the 'NAME' and Credentials must be PRINTED with the signature on the order. A signature log or attestation statement may also be submitted. If the signature is illegible and the name is not printed, the claim will be denied.
- Pre-Admission Screening must be signed by a licensed/certified clinician within 48hrs prior to admission. Narrative information is required, check-off box forms will not be accepted. The IRF physician must review, sign and concur with the screening results. The preadmission screening must include ALL the following requirements:
- Prior level of function (PLOF)
- Expected length of time necessary to achieve expected level of improvement
- Expected level of improvement anticipated
- Anticipated discharge destination
- Anticipated post-discharge treatments
- Eval of the pt's risk for clinical complications
- Treatments needed (e.g. PT/OT/SLP) and expected frequency and duration of treatment while in the IRF
- Documentation of conditions that caused the need for rehab services
- Post-admission physician evaluation previously required was removed but the History and Physical by the rehabilitation physician is still required
- Individualized Overall Plan of Care (POC) signed and dated legibly with the following required components completed within the first 4 days of IRF admission. Documentation must support the following requirements:
- Individualized to the unique circumstances and care needs of the patient
- Estimated length of stay
- Medical prognosis
- Anticipated interventions, functional outcomes, discharge plans and destination
- Therapy details (e.g. intensity (# of hours per day), frequency (# days per week), duration (total # of days during IRF stay)
- Patient requires active/ongoing multiple therapy disciplines (physical therapy, occupational therapy, speech-language pathology, or prosthetics/orthotics), one of which must be physical or occupational therapy
- Minimum 3 hours daily therapy at least 5 days per week, or minimum 15 hours therapy within 7-consecutive day period, beginning with IRF admission date
- Admission Orders
- IRF Patient Assessment Instrument (IRF-PAI) that corresponds with information in the medical record
- Address any discrepancies in the documentation
- Interdisciplinary team conference (ITC) meetings held a minimum of once per week
- must be led by the rehabilitation physician
- provides an assessment of the pt's progress towards the rehab goals and any revisions to the treatment plan required
- IRF physician and ALL required interdisciplinary team members from each treatment discipline must be present at these meetings.
- (e.g. MD, RN, CM and/or SW, and the disciplines PT, OT, ST involved)
Please visit:
Providers may include an outline or cover letter with their documentation. This can be used by CGS Medical Review staff as an Index, and prove very helpful to provide the location of key documentation that supports payment of the claim. However, the cover letter cannot be used as documentation, and the documentation must support the contents of the cover letter in order to be useful.
In addition, providers may use brackets, such as [ ] or { }, asterisks (*) or underlined text in the documentation to draw the reviewer's attention to important information. However, notations should not alter, or give the appearance of altering, the documentation. The use of a highlighter is not recommended as documentation may not be legible.
We encourage all CGS providers to utilize myCGS Portal, a free service available 24/7, which offers access to beneficiary eligibility, claim and payment information, forms allowing you to submit redetermination requests, and respond to Medical Review Additional Documentation Requests (ADRs) and much more. Please enroll for myCGS if you have not already done so.
Check the Calendar of Events to sign up for any webinars that may be of interest.
Please contact J15APROBEANDEDUCATION@CGSADMIN.COM for further questions, concerns, or educational needs related to the TPE process. Be sure to include the facility name and Provider number/PTAN for the inquiry. Ensure CGS is current with provider contact information for any educational outreach opportunity.
